
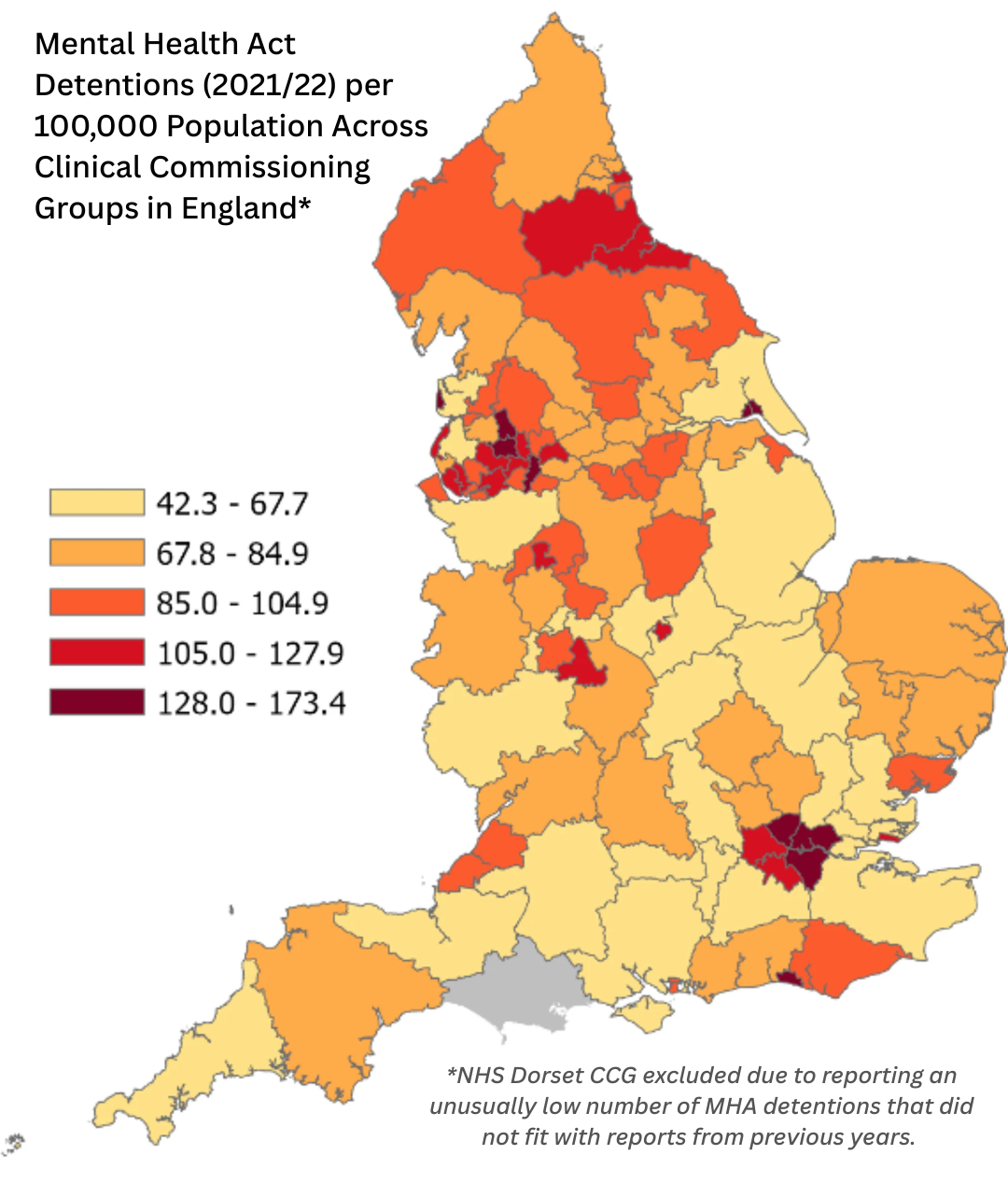
Why Are MHA Detention Rates So Different Across England? A Closer Look for AMHPs
In this blog, I will discuss the above study which I conducted with a team at UCL, looking at variation in the rates of Mental Health Act (MHA) detention across England. Using data from 2021/22, we found a four-fold difference between the areas in England with the highest and lowest rates of MHA detention. Only 11% of this variance was explained by the demographic and clinical variables we used in our study, the rest being unexplained. I wanted to share these findings with AMHPs as the professionals making these decisions, so we can think about why we are seeing this variation. I’ll first share some research that has looked at variation in use of the MHA across England. I’ll then talk about our study and what we found in more detail.
CTOs: “Should they stay or should they go?”
“It's always tease, tease, tease…..”
Reading over our mini blog series and the other editors’ comments, I’m inclined to agree with one of the prevailing themes. The 2025 amendments (now in statute as of the 18th December 2025) feel like something of a missed opportunity. And, there is no better case for this than with a certain section of the Act that has long been in the crosshairs for reform or, indeed, outright abolition; Community Treatment Orders (CTOs) (s.17a) introduced during the last round of amendments in 2007. Initially designed to reduce the number of admissions for the so-called ‘revolving door’ patient and to improve community engagement, they have since proved divisive and achieved a position of some notoriety - to say the least.

A time for change, and a time to choose: the law of unintended consequences.
The new Mental Health Act 2025 gained royal assent on 18th December 2025, some 7 years after the governments intention to modernise the Mental Health Act was unveiled in the King’s Speech in July 2017. The question I have asked myself is whether this is the new legislation in its entirety that we ultimately needed. Our mental health law has once again progressed through a process of evolution rather than revolution. Nonetheless, we now have the 2025 Act which will amend once again the 1983 Act, and we are awaiting the new accompanying Code of Practice and other secondary legislation. Despite this I will share some of my musings about the anticipated ‘Nominated Person’ role which is to replace the outdated role of the ‘Nearest Relative’ as relevant to civil provisions of the Act.

MHA Reform and the Invisible AMHPs: Why ethical and relational AMHP practice is absent from the Bill
As I write, the Mental Health Bill is in its final ‘ping-pong’ stage between the House of Lords and the Commons and is expected to receive Royal Assent in the coming weeks. Here at the Critical AMHP blog, we are publishing a short series that critically examines the reforms through an AMHP lens: the good, the bad, and the indifferent. For my part, I represent the indifferent. I feel like the Bill should matter—certainly it is overdue. So why, then, do I feel so indifferent?

Reform into Renewal: how social care and community services can seize the opportunity for change
Cast your mind back to 2016 when Theresa May made her inaugural prime ministerial speech outside Downing Street about the ‘burning injustices’ of our age…do you vaguely remember? To be fair, since then a LOT of other stuff has gone on in and around that most famous of UK addresses - but it was quite something that a prime minister chose to include the ever-increasing use of compulsory Mental Health Act powers as one of her priority issues for government during that all important opening period in office. Eight years, a costly Independent Review, and considerable expert-by-experience, professional and political debate later, will the stricter detention criteria and some of the other reforms contribute to a reduction in compulsory admissions and address the disproportionate use of compulsion amongst some racialised communities, as it was intended to do?

Guiding Principles and the status quo
As part of s. 118 (1) of the MHA there is a contemporary code of practice to guide doctors, approved clinicians, AMHPs and others in relation to hospital admissions, guardianship and community orders. This code needs to include a statement of guiding principles which should inform decisions under the Act (s.118 (2A)) and to which these professionals must ‘have regard’ (s.118 (2D))

Sexy Cinderella: A Quest for a 28-Day Lie Down
An AMHP’s tale from the frontline of delusion and decision paralysis. Part satire, part case study, and entirely true - a darkly funny reflection on what happens when systems crumble, beds disappear, and the AMHP is left holding the hot potato. All names, locations, and identifying details have been changed or altered to protect confidentiality.
Featuring a barefoot prophet, a surprise cameo from Vladimir Putin, and a haunting rendition of Sexy Cinderella, this story peels back the curtain on the surreal, maddening, and occasionally moving world of Mental Health Act assessments.
Because when no one else knows what to do?
They call an AMHP.

We might have always done it, but we can now explain it – responding to Tim Gorvett’s piece on s13 consideration.
I have sat on my hands for a few weeks, worrying that it might be bad form to respond to Tim Gorvett (SPEAKING IN PROSE & THE REDISCOVERY OF S.13(1) MHA 1983 — Blog Home) when it is obviously for John Mitchell and Robert Lewis to have their right of reply.
But we AMHPs aren’t supposed to be deterred by bad form, nor any nascent feelings of inadequacy regarding our expertise in French literature! Let me aim to be one of those energetic and creative AMHPs that Tim talks about in his closing comments, and send in my thoughts, for what they are worth… Here goes.

SPEAKING IN PROSE & THE REDISCOVERY OF S.13(1) MHA 1983
John Mitchell and his colleagues have noticed (see the Introduction:4/4 of the 2024 Discussion Paper – reference below) that their recent rediscovery of s.13(1) of the MHA has not met with universal enthusiasm, and they have wondered why this is, laudably calling for wider debate and for critical views to be expressed. Before doing so, it is worthwhile taking a moment to consider why this might be so.
If colleagues are chary of contending in this matter, it may be because the arguments being made so far succeed too well, after all. They are in favour of reducing compulsory admission, of moderating the terrible impact on the global majority population, of taking more quality time on assessments and maximising alternatives to admission, of making our lives as AMHPs easier and more satisfying, and this appears to be the means to these ends. It can come to feel as if to differ is to be arguing against motherhood and apple-pie, against everything that an AMHP stands for. I feel a bit nervous myself.

Critical AMHP Interview with Vincenzo Pasante on the Trieste Model and Statutory Practice in the UK.
Vincenzo has been a service user in Trieste as a teenager, before studying psychology and then gaining experience as a volunteer and as an intern in different services in the city. He moved to the UK in 2014 and has since worked in a number of roles, including in NHS mental health crisis services. In 2019 he started "A Place of Safety?" podcast and has been engaging in an ongoing uphill struggle to bring Basaglian ideas and practice to the UK

Views on the AMHP contribution to Mental Health Act assessments
There is much we can learn as AMHPs about our professional practice from the feedback we get from third parties. I have had an interest in this area throughout my professional career. For many, our exposure is limited to when such feedback comes from an AMHP in training and on their practice placement. As assessors, are we satisfied the person has been interviewed ‘in a suitable manner’? And, has there been meaningful engagement with the Nearest Relative such that a next steps decision based on ‘all the circumstances’ present [S.13 (2) Mental Health Act] can be made? As AMHPs we are indebted to the late Matt Simpson for reminding us that the proper and effective use of S.13 does not automatically lead to a mental health hospital admission outcome, nor should it.

AMHP efficiency and Jevons paradox
The recent release of the Chinese AI chatbot DeepSeek caused some significant waves in the tech industry, not least because the market value of American tech companies plummeted. DeepSeek has seemingly upended many of the assumptions regarding the resources and funding required to produce the next generation of AI. Drawing parallels with the US-USSR space race, many observers described it as AIs sputnik moment (Milmo et al. 2025; Roose and Newton 2025). Amidst the panic however, Microsoft CEO Satya Nadella attempted to put a positive spin on the situation by referencing a 160-year-old economic theory; Nadella posted on social media “Jevons paradox strikes again! As AI gets more efficient and accessible, we will see its use skyrocket, turning into a commodity we just can’t get enough of.”

Taking a “Cheeky Look” at Case Records: Balancing Curiosity and Ethics in AMHP Practice
As a social worker and social researcher, my journey has been filled with many eye-opening discoveries. During my PhD in Social Policy and Social Work, funded by the Economic and Social Research Council, I explored the disproportionate involuntary detention of Black people under the Mental Health Act (MHA). I thought I had a solid grasp of the complexities involved in Approved Mental Health Professional (AMHP) practice. However, an unexpected finding emerged: what I now call the ‘cheeky look phenomenon’ (Aleong, 2023).

A Neurodevelopmental Perspective on Navigating Section 136: How Can Police Officers and AMHPs Help Reduce Distress?
Having been (inappropriately) detained on a number of occasions under Section 136 of the Mental Health Act, without reasonable and practical steps taken to assess whether I lacked capacity, I aim in this blog to suggest steps and guidance for professionals when faced with autistic people in suicidal distress.

Warrantlessness
When it finally happened, it was a very matter of fact process. I notified the relevant people in the Council. My letter contained genuinely heartfelt thanks, followed by confirmation as to what I would do with relevant proof of role. I am indeed talking about handing in my warrant. As of today, I am no longer an Approved Mental Health Professional. Rest assured as an ex-AMHP I don’t go to the Mental Health Act equivalent of the House of Lords; I simply continue being what I am – what I love being and what am proud of being – a Social Worker.

S13 Consideration and Solution Focused Practice – further reflections on a very good fit.
The more I use Solution Focused Practice in my AMHP work, the more I see its very good fit with the kind of s13 consideration that we have been talking about so much recently in AMHP circles. This is, of course, entirely due to the hard graft of Robert Lewis and John Mitchell, and the recent launch of their eBook, in memory of the work of Matt Simpson.
And it's for this reason that I have sent in another blog, in quick succession to my April offering, because I want to do two things. First, to put a spotlight on paragraph 17 of the eBook; and then to talk about a recent piece of Mental Health Act work with a young adult held under s136.
AMHP reapproval and ‘relevant training’: A tokenistic tick-box exercise, or an opportunity for critical and radical engagement?
As AMHPs, we are all aware of our statutory requirement to complete a minimum of 18 hours annual training which has been agreed with the approving Local Social Services Authority (LSSA) as being relevant to our role as an AMHP. I recently undertook some research into the issue of AMHP re-approval (see Mearns, 2023) and this experience really made me think critically about the issue of ‘relevant training‘. How do I feel about my annual AMHP refresher? Do I see it as an administrative-bureaucratic tick-box exercise - “what, legal update……again”? Or does it make me genuinely feel inspired and motivated, a real opportunity to set my own training agenda and reconnect with core AMHP values, to improve my practice in terms of ethical, antiracist and practice-focused solutions?

The Road to Research
By Jenny Daly
I’ve been working as an AMHP in London since 2019. Prior to this, I had never imagined myself as an AMHP, I’d been working as a social worker in a community mental health team for five years. At which point I found I was next in line to go on the AMHP training. Despite my ambivalence about being an AMHP, once I started the training, I enjoyed the learning experience immensely. I remember one of our teachers compared the AMHP role to a human rights champion for the person being assessed. On getting through the course, I was added to the local AMHP duty rota on top of my social work role. I continue to practice as an AMHP about once a week.
Thinking Differently About the Mental Health Act
The discussion paper “‘MHA Assessments’ and s13(1) MHA 1983” challenges many of our core assumptions about what a ‘Mental Health Act assessment’ actually is, as well as examining the role of the Approved Mental Health Professionals who co-ordinate the process. The suggestion here is that our way of assessing people may itself contribute to excess detentions: that changes to AMHP practice are required, and to the organisation of AMHP services, if we are to detain fewer people.

s13 Consideration and Solution Focused Practice – the ‘why’ and the ‘how’?
I never had the privilege of meeting with, or talking to, Matt Simpson, for whom the recent AMHP Leads Conference was a dignified and quietly emotional tribute. From what people have said about him, and his way of working, I think he would be very pleased if AMHPs continued to wrestle with his writing about s13 consideration and practice, in a critical way.
Barbara Swan in her recent post on here reflects both on Matt’s work and her own sense that there are systemic pressures on AMHP autonomy. She says Matt’s article – Changing Gears and Buying Time, published in the British Journal of Social Work in early January 2024 – ‘explores AMHPs decision making at the point of referral and offers a different way of working which is thoughtful, comprehensive, strengths based and person-centred’.